.jpg)
Is Your Pelvic Pain Actually Coming From Your Spine?
- Gaia Women's PT and Wellness

- Jul 1
- 6 min read
Updated: Jul 2
If you have pelvic pain, you've likely you may have consulted with numerous physicians to figure out the root cause of your symptoms. You've been told everything looks normal, but the pain, pressure, or tension in your pelvis is very real and it's not going away. If this sounds familiar, there's a piece of the puzzle that often gets missed entirely: your spine and the nerves that come from it.
Pelvic pain is one of the most under-diagnosed and undertreated conditions in women's healthcare. It also happens to be the most reported conditions that we treat at our clinic.

The Many Causes of Pelvic Pain (And Why None Should Be Overlooked)
Pelvic pain can be challenging to diagnose, partly because so many different systems can contribute to it. It can result from conditions like endometriosis or interstitial cystitis, from overactivity of the pelvic floor muscles, from structural issues like fibroids or prolapse, or from complex pain conditions like vulvodynia. A thorough workup matters, because the source isn't always obvious and it isn't always singular.
Getting to the root of pelvic pain means taking all of it seriously. And that includes something that rarely makes it onto the list: the spine.
Your Symptoms Tell a Story
Someone who knows how to listen can follow that story all the way back to where it started, whether that's in the spine or somewhere along the path a nerve takes to get there.
Here's what most people don't realize: nerves don't just connect one point to another. They travel long, winding routes through muscle, bone, and tissue before they reach their destination. A nerve that originates in your lower back passes through your hip, your deep gluteal muscles, and into your pelvis before it even gets to the structures you feel symptoms in. Anywhere along that route, things can go wrong. A disc can press on a nerve where it exits the spine. A tight muscle can compress it as it passes through. Scar tissue, inflammation, or joint dysfunction can irritate it mid-course.
The result? Pain, burning, pressure, or dysfunction that feels like it's in your pelvis, with no obvious source in sight. This is why pelvic PT isn't just about the pelvic floor. It's about understanding the entire pathway.
When the Problem Is the Nerve, Not the Destination
There are nerves that show up over and over again in cases of pelvic pain that hasn't fully responded to treatment. Each one has a distinct symptom pattern, and recognizing that pattern is often the first step toward finding an answer.
Pudendal Nerve
The pudendal nerve is responsible for sensation in the vulva, clitoris, perineum, and anus, and controls the urethral and anal sphincters. It travels from the lower sacrum through the greater sciatic notch, wraps around a ligament, and runs through a narrow tunnel along the inner wall of the pelvis before branching out to its final destinations.
That's a long trip with several places where things can get compressed or irritated.
When the pudendal nerve is involved, symptoms often include:
Burning, stabbing, or aching pain in the vulva, clitoris, urethra, perineum, or rectum
Pain that is worse with sitting and better with standing or lying down
A sensation of something being inside the vagina or rectum when nothing is there
Pain during or after intercourse
Urinary urgency, frequency, or feeling like the bladder doesn't fully empty
Pain or difficulty with bowel movements
Obturator Nerve
The obturator nerve travels from the lumbar spine down through the pelvis and out through a small opening in the pelvic bone to supply the inner thigh muscles and skin. Because it passes directly through the pelvis, dysfunction along its path can be easy to misread as a gynecological issue.
Obturator nerve involvement often looks like:
Deep groin or inner thigh pain that's hard to pinpoint
Pain when crossing your legs or squeezing your thighs together
A vague sense of pelvic heaviness or achiness
Discomfort that feels like it could be ovarian but isn't cycle-dependent

Sciatic Nerve
Most people know the sciatic nerve as the source of that shooting pain down the back of the leg. What's less known is that it also has meaningful connections to the pelvic floor, and that the muscle it passes directly next to, the piriformis, is one that pelvic floor patients tend to hold a lot of tension in.
When the sciatic nerve is involved in pelvic pain, it can present as:
Deep aching in the buttock that extends into the pelvic floor
Posterior pelvic pain that feels internal
Pain with sitting, especially on firm surfaces
Symptoms that get worse with prolonged walking or hip movement
The sciatic nerve travels under or through the piriformis muscle and then down the back of the pelvis and hip. This nerve, or branches of it can be the source of pelvic pain in the pack of the pelvis and even near the tailbone and rectum.
Ilioinguinal Nerve
The ilioinguinal nerve travels from the upper lumbar spine through the lower abdominal wall and into the groin, inner thigh, and labia. It's a nerve that rarely comes up in conversations about pelvic pain, but it's responsible for sensation in areas where women commonly report symptoms that get attributed to other things.
When the ilioinguinal nerve is irritated, symptoms can include:
Burning or aching in the groin or inner labia
Numbness or hypersensitivity along the inner thigh
Pain or tenderness at the lower abdomen near the bikini line
Symptoms that worsen with prolonged standing, walking, or hip extension
This nerve is particularly vulnerable in women who have had C-sections, hernia repairs, or other lower abdominal surgeries, as scar tissue along its path can compress or tether it over time.
Genitofemoral Nerve
The genitofemoral nerve follows a similar route but branches to supply sensation to the mons pubis, labia majora, and upper inner thigh. Because its territory overlaps with areas commonly associated with vulvar pain conditions, irritation here is frequently mistaken for vulvodynia or a localized skin condition.
When the genitofemoral nerve is involved, symptoms can include:
Burning or crawling sensations at the mons pubis or labia majora
Sensitivity or numbness along the upper inner thigh
Discomfort that feels superficial but doesn't respond to topical treatments
Pain that shifts or spreads depending on posture or activity
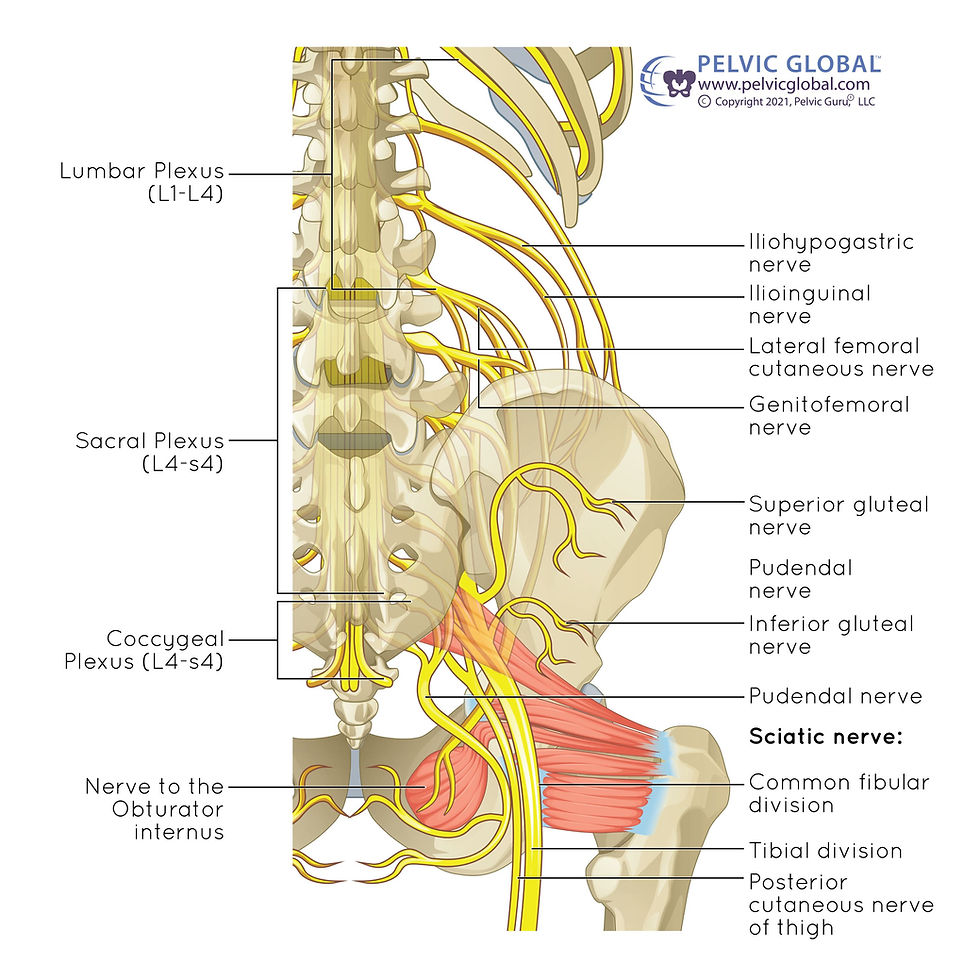
Where Do These Nerves Come From?
All of these nerves originate in the lower lumbar spine and sacrum, roughly from the L1 through S4 spinal levels. Think of those levels as the source, and the nerves as the branches that carry information out to the pelvis.
Problems at the source affect everything downstream. A disc herniation at L4-L5 can irritate the nerves before they even leave the spine. Sacroiliac joint instability can compress the sacral nerves at their origin. Tight hip flexors can pull on the lumbar spine in ways that gradually sensitize the nerve pathways below.
This is also why pelvic symptoms sometimes flare alongside low back pain, and why women with a history of sciatica or disc issues are often surprised to learn their current pelvic symptoms may be related.
Could This Be What's Happening for You?
There's no single test that confirms a spinal or nerve contribution to pelvic pain, which is part of why it goes undetected for so long. But certain patterns are worth paying attention to:
Your pain changes depending on how you're sitting, standing, or moving
You have a history of low back pain, sciatica, or disc issues, even if those symptoms have calmed down
Your pelvic symptoms are somewhat predictable based on your activity level or posture
Standard pelvic treatments have helped somewhat but never fully resolved things
You also notice hip, gluteal, or tailbone discomfort alongside your pelvic symptoms
Heavy lifting, running, or prolonged sitting reliably makes things worse
None of these on their own confirms anything. Together, they tell us something worth following.
What We Look For at Gaia
When you come in with pelvic pain, we're not only assessing the pelvic floor. We're looking at the whole system, because the source of your symptoms may be nowhere near where you feel them.
A thorough evaluation may include assessing lumbar and sacral mobility, testing the sacroiliac joints, evaluating how the piriformis and hip muscles are functioning, checking whether specific nerves appear sensitized or restricted in their movement, assessing internal pelvic floor tone and tenderness, and looking at how you move and hold your body throughout the day.
That full picture is what makes it possible to find answers that a more limited evaluation would miss.
You Don't Have to Keep Starting Over
If you've been living with pelvic pain and feel like you've worked through every explanation, it may simply be that no one has looked at the whole pathway yet. That's not a failure of your body or your previous care. It's a gap that we see often, and one we know how to address.
Contact us to schedule an evaluation at Gaia Women's Physical Therapy in Martinsburg, WV.